


This is part two of our series on lessons learned from our time at the American Epilepsy Society in December 2023. You can read Part 1 here.
Families and clinicians have a lot of hurdles to overcome in genetic testing for epilepsy.
For the past two years, the Child Neurology Foundation has hosted a half-day summit on genetic testing. This year’s session was hosted by Dr. Scott Perry, from Cook Children’s Hospital in Texas, opened the session by sharing results from a 2022 survey conducted by the Child Neurology Foundation, revealing that 40% of families did not know the reason for their child’s epilepsy and a third had never had genetic testing.
Some clinicians push back on genetic testing, arguing that it won’t lead to a diagnosis or treatment options. Perry argues that families are dealing with the heavy lift of having to care for children with these disorders every day. “Simply knowing your child has epilepsy is not the end of the road. Knowing what the disorder is and being able to connect with other people that have that disorder is treatment – whether there is medication for it or not. Knowing who your community is, if nothing else, can connect these families to disease-specific connections important to the family.”

Parent dilemmas
Tristin West, a parent, spoke about her family’s epilepsy journey. Her son has a rare mutation with only 30 known patients. She said that before genetic testing, her son didn’t matter, but finally, he mattered when his genetic mutation was discovered because researchers wanted to find the patients with this disorder and write about them. “We were told that a diagnosis wouldn’t make a difference, and it’s made all the difference in the world. Maybe if we were to write it down scientifically, clinically, maybe not. But we have learned so much by having a diagnosis, and we have a community now. There’s a huge ripple effect. It affects generations. It leaves a medical legacy. It saves lives. It literally changes everything in the lives of our families.”
Clinical dilemmas
Dr. Christa Habela and Krista Schatz from Johns Hopkins University shared that, until last year, there were no formal recommendations in regard to genetic testing and epilepsy. Now, for the first time,new practice guidelines from the National Society of Genetic Counselors and endorsed by the American Epilepsy Society recommend genetic testing for everyone with epilepsy, regardless of age.
- Neurologists and epileptologists should make genetic testing part of routine clinical practice.
- Recommended testing is whole exome or whole genome sequencing as the first line test and then reflexing to chromosome microarray. If the whole exome or whole genome is unavailable, the recommendation is to start with a large multi-gene panel.
They also pointed out that genetic diagnoses and surgical management of epilepsy are interrelated. For example, patients with somatic changes in genes associated with the mTOR pathway are likely to respond better to surgery than those who have channelopathies. So, genetic testing can help plan surgical or other treatment options.
Genetic Testing in the Transition to Adult Care
Dr. Danielle Andrade of the University of Toronto (and Co-Chair of the ILAE Transition Task Force) highlighted some reasons for genetic testing:
- Guilt – Many caregivers, especially mothers, have always wondered, “Why?” But when they found a genetic diagnosis, they said, “So this is not about the wine I had when I didn’t know I was pregnant yet?” Mothers carry guilt for many years that they might have done something bad to their child. So, learning why and getting rid of the guilt is an important reason to have a genetic diagnosis.
- Treatment adjustments – Some conditions have specific medications that work best.
- Family planning, even for siblings – The adult sibling of a patient with epilepsy might be worried about starting their own family, especially if there is no diagnosis. A diagnosis may give some comfort or information to help them decide whether or not they want to have children. Or, if the mother of a child with epilepsy is still of childbearing age, she may want to have more children as well.
- Understanding the natural history of a disease – When you start seeing many adults with a condition, you can learn what will happen to children with this particular mutation when they grow up.
Dr. Andrade is an adult neurologist, and she discussed the difficulties of transitioning to adult neurological care with or without a genetic diagnosis. She explained that adult neurologists are often not familiar with genetic conditions.
In the past, a child neurologist would see a patient with apparent genetic epilepsy and do “The $1 Million Workup,” including metabolic tests, fish, karyotype, and biopsies – all that was available. If there were no diagnosis, this patient would move to the adult neurologist with a diagnosis of “asymptomatic generalized epilepsy.” Now, there are newer genetic tests so that patients may have had a panel, exome, or even genome sequencing yet are still transitioning to adult care without a diagnosis. So, many adult neurologists will say, “They did everything possible on the pediatric side; I’m not going to find anything. I’m going to stop investigating any genetic cause. I’ll focus on treatment.”
Even if the adult neurologist pursues genetic testing, it’s challenging when they find a new gene in an adult patient. Most of what they will read about this gene was written by child neurologists, describing what happened to patients as children. Adult neurologists might also not have access to the patient’s medical record or may not have time to read the entire chart.
The adult neurologist may also not be trained to treat patients with genetic epilepsies. If your child has a genetic diagnosis and transitions to an adult neurologist who has never heard about this condition (that’s usually what happens, according to Dr. Andrade), what do you do?
This is where a planned transition to the adult side is very important. The pediatric neurologist should make a “knowledge transfer” to the adult neurologist and help the family feel safe and secure while transitioning to a new clinician. Communication between pediatric and adult providers is extremely important.
When a pediatric patient is transferring to an adult neurologist, Dr. Andrade recommends that the child neurologist summarize the whole course of the child’s care and provide some literature to the new neurologist. It’s very important that the child neurologist sends to the adult neurologist a proper transition letter or transfer letter listing all types of seizures that happened in the past, response to medications, treatments, or ketogenic diet, etc., and document what genetic testing was done, the results, or if there was a variant of unknown significance (VUS). Even if the child is not diagnosed with genetic epilepsy (yet), it’s essential to have a proper history of when the patient was growing up. If genetic epilepsy is suspected, the child neurologist can state, for example, that “the investigations should be repeated in two or three years until a cause is found because this is very likely a genetic diagnosis.”
![]()
Possible challenges when transitioning a pediatric patient with genetic epilepsy to adult neurology:
- The availability of an adult neurologist knowledgeable of the condition.
- Difficulty finding a neurologist to see the patient because their practices are full.
- The comfort level of adult neurologists – many are uncomfortable treating patients with genetic epilepsies, not only the seizures but all the comorbidities that come with it.
- The patient and family have established trust with the child’s neurologist, the child has been followed for a long time, and their neurologist knows everything about them: complications, medication reactions, what has been tried before, etc.
- The patient might be too complex for the adult system and feel they will not have the same support they had in the pediatric system. Usually, the child neurologist looks after the child’s seizures, sleep, behavior, and more. They may have a group of physicians they can send their patients to, often in the same hospital. The family sees the right specialists in a closed environment, and the clinicians all talk to each other. The adult system is completely different: if you need a sleep study, that will be a challenge, and if you need an adult psychiatrist to treat a nonverbal patient, that is going to be a considerable challenge. If the patient is on a ketogenic diet and doing well, where in the adult system can you find a keto diet program?
- Sometimes, patients and families have limited medical literacy, so they may have difficulty understanding the value of genetic testing.
Patients and caregivers must be informed that if the child had a genetic test in the past that was negative, it doesn’t mean this is not a genetic disease. Adult neurologists should consider undiagnosed genetic epilepsies and should re-investigate with the new technology we have now and repeat testing every two to three years. Even if there is no current treatment for genetic epilepsy, you might learn about comorbidities, family planning for the adult siblings, or modified or repurposed drugs for this condition. Once we have a diagnosis, we can look for new treatments.
Treatment Dilemmas
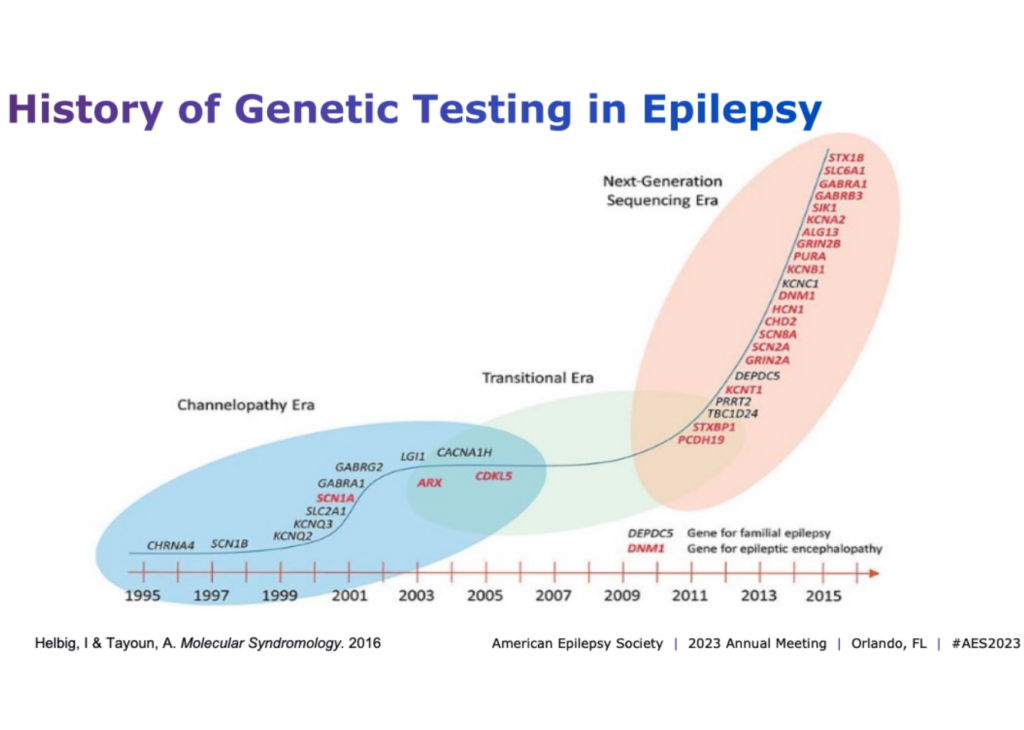
Dr. Scott Demarest of Children’s Hospital Colorado spoke about the fact that there are more than 860 genes now associated with epilepsy. In the past decade, our understanding of genetic epilepsies has exploded. While each gene may have a very low yield, they collectively provide thousands of answers for families.
He discussed the value of genetic testing:
- Regardless of whether there’s a treatment approach, you have a diagnosis or at least a name that you can put on it. It gives hope that there is a direction you can go. Many families have taken this on beyond all expectations and started their own organizations to drive research in this space.
- Testing is more likely to show genetic epilepsy in children. Still, even with onset at an older age or with normal development, regardless of MRI findings, there is a yield to genetic testing. It’s even higher when there are developmental anomalies associated with the MRI.
- There may be published care guidelines associated with those genes for other things we need to consider or monitor besides epilepsy. Epileptologists care about stopping epilepsy, but sometimes, we have to think about the other issues that might come with these genes as well, such as behavioral challenges, developmental delay, communication, GI issues, sleep, or motor impairment. We should aim to improve most symptoms, not just seizures.
- Genetic testing overall is going to lead to treatment via gene therapy. If we fast forward five years, we’re going to have hundreds of patients across the country being treated by epilepsy disease-modifying therapies.
He also talked about setting realistic expectations for families in that we may not cure the underlying condition but can alter the course of the disease. We also need to be candid about the potential risks of these new therapies, things we don’t know about yet. These conversations become complicated, and we need to learn how to do these well as a community.
Meeting recap
Dr. Sarah Kelley from Johns Hopkins Hospital summarized the meeting. Last year, the session “Genetic testing in epilepsy, improving outcomes and informing gaps in research” covered:
- overcoming barriers to genetic testing for patients;
- the importance of training and getting resources to be able to do this well;
- exciting new techniques available for genetic testing;
- how to use these to address the whole patient and their family.
This year, they wanted to think about the difficult conversations and dilemmas they have in the clinic when doing genetic testing for a patient. In epilepsy research, we are learning more about the value of genetic testing. We can identify so many more genetic changes now, and our knowledge continues to grow.
She highlighted the following points from this session
- the challenges of accessibility of testing, resources, and interventions;
- thinking beyond treating epilepsy, but also treating other aspects of development based on the outcomes that are important to families;
- advocating for patients and families and helping families advocate for their loved ones;
- how to counsel patients on the benefits of testing;
- genetic testing is valuable even in the adult world, from transition of care, treatments available to adult patients, comorbidities that may manifest later in life, or family planning;
- how to address the challenging questions that arise when a diagnosis is made.
You can learn more about this session here, view the slides here, and watch the recording of the 2022 session here.
Stay tuned for my next blog post about another topic we learned about at the American Epilepsy Society annual meeting: mortality in epilepsy.
about the author

Audrey Vernick is our Director of Patient and Family Advocacy. She is the parent of a child who had hemispherectomy for seizures caused by stroke. She holds a level 2 certification in Special Education Advocacy Training from the Council of Parent Attorneys and Advocates and is certified by The ARC in future planning. She also serves on the International League Against Epilepsy’s Social Work and Social Services Section.